2022 Report of the Auditor General of Canada to the Northwest Territories Legislative AssemblyAddictions Prevention and Recovery Services in the Northwest Territories
Independent Auditor’s Report
Table of Contents
- Introduction
- Findings, Recommendations, and Responses
- Ensuring access to addictions prevention and recovery services
- Measuring outcomes for clients
- Conclusion
- About the Audit
- List of Recommendations
- Exhibits:
Introduction
Background
1. The Northwest Territories has some of the highest rates of addictions and substance use in Canada. According to the Government of the Northwest Territories’ 2019–20 annual report on the territory’s health and social services system, indicators such as the rates of smoking and heavy drinking in the territory had not significantly changed over recent years. According to the report, these rates were about 2 times higher and 1.5 times higher, respectively, than the national averages. The report also noted that adults and youth were hospitalized for harm caused by substance use, mainly alcohol and cannabis, at a rate that was over 3 times the national average.
2. The Northwest Territories has a vast geographic area with a population of about 45,000 residents. Slightly fewer than half of its residents live in Yellowknife. About half of the territory’s 33 communities have fewer than 500 residents, and many of these communities are remote and accessible only by plane or winter roads. The vastness of the territory and the remoteness of many communities create challenges for the delivery of addictions servicesDefinition 1. Additionally, roughly half of the territory’s population identifies as Indigenous. It is important for all Northwest Territories residents, including individuals from the territory’s diverse Indigenous cultures, to feel safe and respected when accessing health and social services.
3. Furthermore, social determinants of health—things like housing, education, and involvement with the criminal justice system—can influence whether a person develops an addiction. Indigenous social determinants, including colonization and systemic racism, can also influence addictions. It is important for the health and social services system to consider these factors.
4. For many years, the Government of the Northwest Territories has recognized that improvements are needed to address addictions in the territory. Here are 2 examples:
- In 2012, the Minister of Health and Social Services created a forum to determine the direction of mental health and addictions programs. This resulted in the 2013 Healing Voices report.
- The Department of Health and Social Services developed a 2016–21 framework to strengthen the mental health and addictions system in the territory.
5. Also, in 2015, the Government of the Northwest Territories released Meeting the Challenge of Reconciliation: The Government of the Northwest Territories Response to the Truth and Reconciliation Commission Calls to Action. The response recognized the importance of incorporating Indigenous knowledge into the delivery of health services and the need for health care professionals to have cultural sensitivity training.
6. The Department of Health and Social Services. The Department of Health and Social Services is mandated to promote, protect, and provide for the health and well‑being of the people of the Northwest Territories. The department is responsible for setting objectives and priorities for the territory’s health and social services system. This includes both ensuring that eligible residents have access to health and social programs and services and supporting wellness programs at the community level, including those that help people affected by addictions. The department is also responsible for determining how health and social services resources within the department, including human resources, should be allocated.
7. Health and social services authorities. Three health and social services authorities are responsible for delivering services, including addictions services, in line with the department’s objectives and priorities for the health and social services system (Exhibit 1). The 3 health authorities are as follows:
- the Northwest Territories Health and Social Services Authority, created in 2016 following the amalgamation of 6 health authorities
- the Hay River Health and Social Services Authority
- the Tłı̨chǫ Community Services Agency
These health authorities are responsible for managing their own financial, human, and other resources. The Northwest Territories Health and Social Services Authority conducts strategic human resources planning on the department’s behalf. It is also responsible for operating the Stanton Territorial Hospital.
Exhibit 1—Communities served by the 3 health and social services authorities
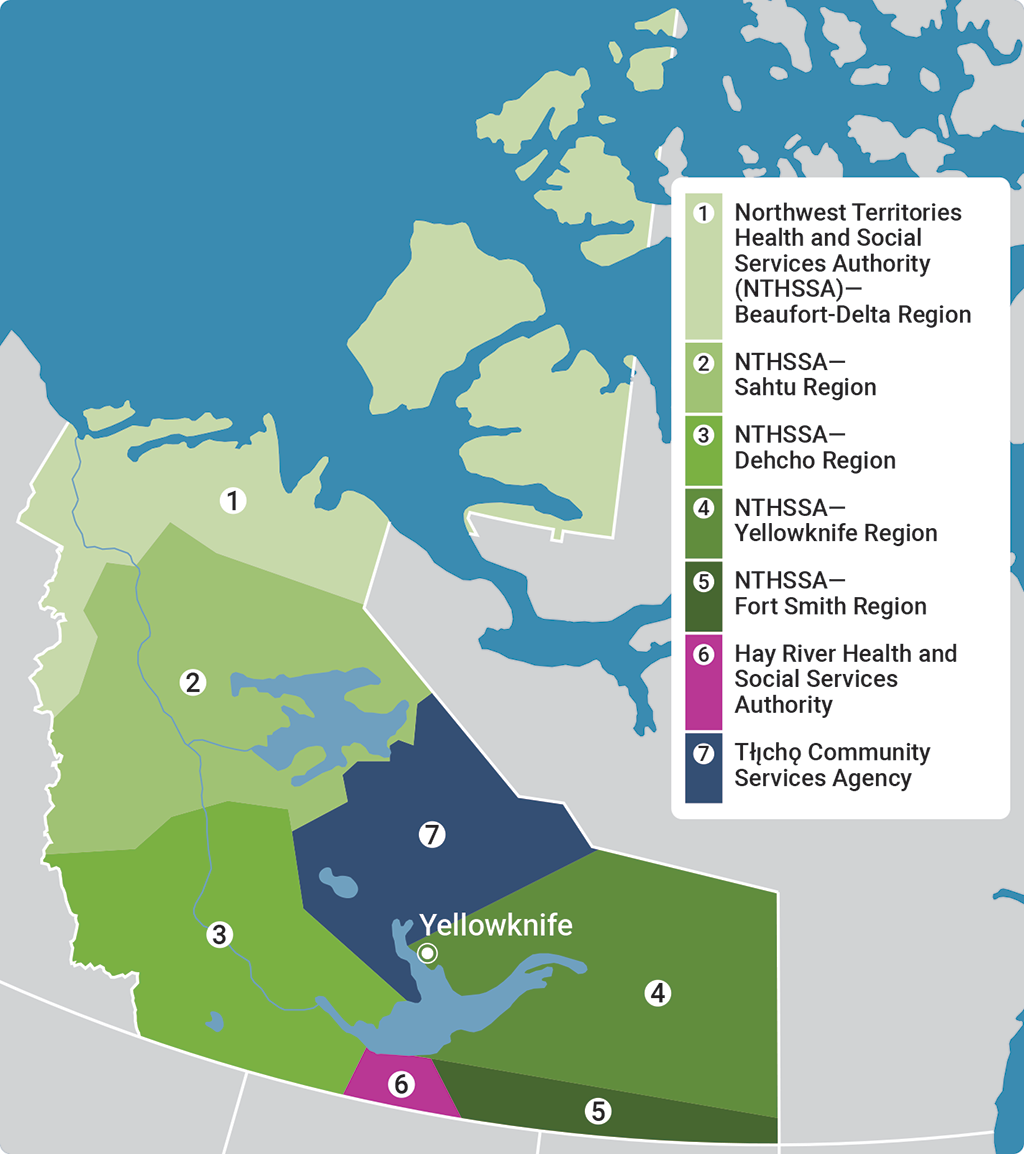
Source: Based on documentation from the Northwest Territories Health and Social Services Authority
Exhibit 1—text version
This map shows the areas in the Northwest Territories served by the 3 health and social services authorities: the Northwest Territories Health and Social Services Authority, the Tłıcho Community Services Agency, and the Hay River Health and Social Services Authority.
The Northwest Territories Health and Social Services Authority is split into 5 regions: the Beaufort-Delta Region, the Sahtu Region, the Dehcho Region, the Yellowknife Region, and the Fort Smith Region.
The Northwest Territories Health and Social Services Authority—Beaufort-Delta Region serves the northernmost area of the Northwest Territories.
The Northwest Territories Health and Social Services Authority—Sahtu Region serves the area directly south of the Beaufort-Delta Region, extending southward to approximately the central part of the territory and stretching across the territory from east to west.
The Northwest Territories Health and Social Services Authority—Dehcho Region serves the southwest area of the territory, directly south of the Sahtu Region and extending to the border between the Northwest Territories and Alberta.
The Tłıcho Community Services Agency serves the area of the territory north of Yellowknife to approximately the central part of the territory, directly east of the Dehcho Region and south of the Sahtu Region.
The Northwest Territories Health and Social Services Authority—Yellowknife Region serves the eastern area of the territory directly south of the area served by the Tłıcho Community Services Agency and north of the Fort Smith Region.
The Hay River Health and Social Services Authority serves the area directly south of Yellowknife along the border between the Northwest Territories and Alberta and between the areas served by the Dehcho Region and the Fort Smith Region.
The Northwest Territories Health and Social Services Authority—Fort Smith Region serves the southeastern most area of the territory along the border between the Northwest Territories and Alberta.
8. Indigenous governments and non‑government organizations. Some addictions services, such as on‑the‑land healing programs, are delivered by Indigenous governments and non‑government organizations through agreements with the department or the health authorities. These groups may also provide services funded by other means, independent of the Government of the Northwest Territories.
Focus of the audit
9. This audit focused on whether the Department of Health and Social Services and the health and social services authorities provided addictions prevention and recovery services to meet the needs of Northwest Territories residents.
10. This audit is important because addictions are a significant concern in the Northwest Territories. Addictions can have serious health and social consequences. They can affect families, education and employment opportunities, social integration, and financial stability. The Northwest Territories health and social services system plays a critical role in providing addictions services to its residents.
11. More details about the audit objective, scope, approach, and criteria are in About the Audit at the end of this report.
Findings, Recommendations, and Responses
Overall message
12. Overall, we found that, despite many commitments, the Department of Health and Social Services and the health and social services authorities did not do enough to provide residents with accessible, coordinated, and culturally safe addictions services. Furthermore, they did not know whether addictions services assisted all residents effectively in meeting their desired outcomes. We found concerning shortcomings in the provision of addictions services, from ensuring equitable access to services for all residents to ensuring that services are culturally safe for Indigenous clients and that aftercare services are sufficient to support clients’ recovery goals.
13. The Department of Health and Social Services and the 3 health and social services authorities have taken some steps to improve services. For example, they have made some adjustments to services to better meet residents’ needs. The department also established the Indigenous Advisory Body to provide advice and guidance on the health and social services system. However, neither the department nor the health authorities had determined how they would provide equitable access to addictions services for all residents across the territory. While we found that addictions services varied over time and by location across the territory, it was not clear whether this was part of the system’s design or due to deficiencies in the system.
14. We were also concerned by a lack of coordination needed to connect clients with the services they required even though it has been 20 years since the department committed to better coordinate the health and social services system to improve residents’ access to services. The department and the health authorities need to do more to deliver on their commitments to provide equitable, culturally safe programs to help people impacted by addictions access the care they need, for their own well‑being and that of their communities.
Ensuring access to addictions prevention and recovery services
The Department of Health and Social Services and the health and social services authorities did not do enough to provide accessible and coordinated addictions services
15. We found that the Department of Health and Social Services and the health and social services authorities had not identified how to ensure that all residents had equitable access to addictions services. This made it difficult to know whether some services could have been more accessible to residents. We also found that there were limited aftercare services to support clients’ recoveries. In addition, we found a lack of system-wide processes to help health authority staff connect clients with some of the services they needed, despite the department’s commitment 20 years ago to better coordinate services across organizations.
16. The analysis supporting this finding discusses the following topics:
- Lack of clarity on how to achieve equitable access
- Limited aftercare support
- Gaps in coordination of services across providers
17. This finding matters because services should be accessible to residents who are seeking help for an addiction. Because various organizations provide addictions services and individuals can enter the system at different points, the system needs to be coordinated to help individuals move through it.
18. Addictions services in the Northwest Territories’ health and social services system focus on the person and their individual goals. Clients play a key role in identifying what services they would like to access and when they are ready to do so. This includes enabling clients to refer themselves to counselling.
19. Addictions recovery is an ongoing process, and people often access services, such as facility-based addictions treatment,Definition 2 more than once. Many services contribute to preventing, treating, and maintaining an addiction-free lifestyle, depending on when the individual accesses them. For example, counselling can help clients develop preventative coping strategies, recover from an addiction, or maintain ongoing sobriety as an aftercare service. Developing an aftercare plan is an important step to help people identify services that will help them to maintain the outcomes that they have achieved.
20. The Government of the Northwest Territories’ 2017–20 strategic plan for the health and social services system includes a guiding principle to ensure equitable access to care and services. Twenty years ago, the department committed to integrating the health and social services system to improve access to services, including those for addictions.
21. Our recommendations in this area of examination appear at paragraphs 30, 31, 35, and 39.
Lack of clarity on how to achieve equitable access
22. We found that neither the Department of Health and Social Services nor the health and social services authorities determined what equitable access to addictions services across the territory would look like in practice. The department and the health authorities also did not identify the actions required to achieve their commitment to providing equitable access to services. As a result, it was not clear whether the fact that the availability of addictions services varied over time and by location was part of the system’s design or due to deficiencies in the system.
23. According to the Government of the Northwest Territories’ 2017–20 strategic plan for the health and social services system, ensuring equitable addictions services would require considering the most vulnerable when developing programs and policies to reduce systemic and avoidable health disparities. Furthermore, the government’s 2016 commitment to building a culturally respectful system indicated that achieving equitable services means that barriers, including geographic remoteness, would not affect the services people seek.
24. We found that the availability of services varied over time and by location across the territory. For example, the Matrix Model, a treatment program designed to address the psychological and educational aspects of addictions, was available only in a small number of communities at any point during our audit period. In contrast, mental health services from trained counsellors were available to all residents through the Community Counselling Program, but residents had different types of access to them: Some communities had resident or visiting counsellors, and others relied on virtual or phone counselling services. Furthermore, other services were launched only recently or were in the early stages of development. This variability meant that some services may not always have been available when residents tried to access them.
25. Even when services were available to all residents, it was not clear whether the system’s design reduced barriers to address health disparities. For example, residents of most communities had to travel to access detox services, which were available on a case‑by‑case basis in Yellowknife, Inuvik, and Hay River or through facility-based treatment centres outside the territory. Additionally, residents wishing to access other facility-based addictions treatment had to leave the territory to obtain this service. Having some services only in certain locations could cause barriers for some individuals, such as those with concerns about treatment not reflecting their culture. The department stated that by entering into service agreements with multiple treatment centres outside the territory, it could maximize the treatment options available to residents.
26. Furthermore, we found that the department and the health authorities did not take sufficient action to ensure that addictions services for Indigenous residents were culturally safe (see paragraphs 47 to 55). Given the legacy of colonization, having culturally safe services is critical to facilitate equitable access for some Indigenous clients.
27. We also found that although the department identified residents’ addictions service needs using several avenues, including forums, community consultations, and client surveys, it did not formally assess the needs of subpopulations, such as refugees or other non‑Indigenous racialized groups. This was despite the department’s recognition in its 2018–20 cultural safety action plan that some subpopulations, including members of the immigrant and refugee communities, expressed that they had challenges accessing care. Without identifying the needs of various subpopulations likely to have increased barriers to access, it is unclear to us how the department and the health authorities could know how to reduce these barriers and equitably meet their needs.
28. Although the Government of the Northwest Territories had not officially adopted the Sustainable Development Goals in the United Nations’ 2030 Agenda for Sustainable Development, our audit aligned with the goal of good health and well‑being (Goal 3) and the related target of strengthening the prevention and treatment of substance abuse, including narcotic drug abuse and harmful use of alcohol (target 3.5). Our findings about equitable access to services indicated challenges related to the coverage of treatment interventions for substance use disorders (indicator 3.5.1). Without equitable access to services, some residents of the Northwest Territories may not have been able to obtain the services they needed to meet their addictions recovery goals.
29. Despite the problems identified, we found that as of September 2020, there were no wait times for initial appointments with a counsellor in 6 of 7 health and social services regions. In our view, it is important that individuals in distress who wish to speak to a counsellor be able to do so. We also found that the department and the health authorities adapted how they delivered services in response to the coronavirus disease (COVID‑19)Definition 3 pandemic. For example, the health authorities ramped up virtual and telephone care for residents wanting addictions services during the pandemic. This included helping people get the technology required to access virtual services.
30. Recommendation. The Department of Health and Social Services and the health and social services authorities, in collaboration with Indigenous governments and communities, should determine how to achieve their commitment to providing equitable access to addictions services in the Northwest Territories, including related timelines, and take the required actions. This should include identifying where and how services should be made available to reduce barriers to access, given the operating environment and related challenges.
The department’s and the health and social services authorities’ response. Agreed.
See the List of Recommendations at the end of this report for detailed responses.
31. Recommendation. The Department of Health and Social Services, in collaboration with the health and social services authorities and relevant stakeholders, should identify the addictions prevention and recovery needs of diverse subpopulations.
The department’s response. Agreed.
See the List of Recommendations at the end of this report for detailed responses.
Limited aftercare support
32. We also found problems with aftercare services for some people who attended facility-based addictions treatment programs in southern Canada. We reviewed files from a random sample of 32 clients who attended a program between 2018 and 2021 following a referral through the Community Counselling Program. We tested the aftercare planning and services that the health authorities were required to provide to these individuals. We found that the health authorities did not provide the aftercare supports that their clients needed to support their recovery goals (Exhibit 2).
Exhibit 2—Health and social services authorities often failed to provide required aftercare support for a sample of clients who attended facility-based addictions treatment programs
| Requirements | Incidence of finding | |||||||
|---|---|---|---|---|---|---|---|---|
| Hay River Health and Social Services Authority | Northwest Territories Health and Social Services Authority | Tłı̨chǫ Community Services Agency | Total | |||||
| Fort Smith | Yellowknife | Beaufort‑Delta | Dehcho | Sahtu | ||||
| Aftercare plan created before clients went into a facility-based addictions treatment program (and application indicated it was done) | 0 out of 5 clients | 2 out of 5 clients | 0 out of 3 clients | 0 out of 5 clients | 0 out of 5 clients | 0 out of 5 clients | 0 out of 4 clients | 2 out of 32 clients |
| Client offered the aftercare services identified as required | 3 out of 3 clients | 3 out of 5 clients | 2 out of 3 clients | 2 out of 5 clients | 2 out of 4 clients | 2 out of 4 clients | 1 out of 3 clients | 15 out of 27Note 1 clients |
| Attempts made to contact client following treatment | 5 out of 5 clients | 2 out of 5 clients | 2 out of 3 clients | 2 out of 5 clients | 3 out of 5 clients | 2 out of 5 clients | 3 out of 4 clients | 19 out of 32 clients |
|
Source: Based on documentation from the health and social services authorities |
||||||||
33. Our finding that aftercare plans were created for only 2 of the 32 clients whose files we reviewed was particularly troubling, especially because all 32 applications indicated that they had been created. Health authority officials told us that aftercare planning was done informally and was documented throughout the client’s file in case notes. Having documented plans that the clients agreed to before treatment could help the counsellors and clients prepare strategies and services that could support clients when they returned home. Aftercare plans could also facilitate continuity of care if there was a change in counsellor. While we saw many examples of counsellors identifying clients’ needs after their treatment in southern Canada and offering help in response, the unavailability of services sometimes limited the referrals that counsellors could make.
34. We also found that in the 2019–20 fiscal year, the Department of Health and Social Services increased the On the Land Healing Fund from $1.2 million to $1.8 million annually to help Indigenous governments and non‑governmental Indigenous organizations to improve land‑based addictions treatment, including aftercare programming. However, some Indigenous groups told us that administrative requirements made accessing the fund difficult. We found that the fund’s budget was not always exhausted: The unspent funds during the period covered by our audit ranged from $20,000 in the 2016–17 fiscal year to $624,000 in 2019–20 fiscal year.
35. Recommendation. The Department of Health and Social Services and the health and social services authorities should
- develop a standard approach to aftercare planning
- ensure that clients who attend facility-based addictions treatment programs have an aftercare plan before they leave for treatment
- facilitate access to aftercare services needed when clients return to the Northwest Territories
The department’s and the health and social services authorities’ response. Agreed.
See the List of Recommendations at the end of this report for detailed responses.
Gaps in coordination of services across providers
36. We found that gaps remained in coordination 2 decades after the Department of Health and Social Services made a commitment to better coordinate the health and social services system to improve residents’ access to services.
37. There were gaps in the processes to help health authority staff understand how they could connect clients entering the system at different access points to the addictions services provided by various organizations. For example, we found that none of the health authorities had established a process for counsellors to help clients move from the Community Counselling Program to services offered by Indigenous governments. A formal system-wide referral process was in place only to coordinate services for individuals requesting access to or returning from facility-based addictions treatment. However, we also found that the Hay River Health and Social Services Authority and the Tłı̨chǫ Community Services Agency had established processes to refer clients to the Community Counselling Program from service providers under these health authorities.
38. We found that the department and the health authorities took some steps to improve coordination by establishing interdisciplinary positions, locating counsellors with other health services, and creating discussion forums. However, counsellors were only co‑located on a part‑time basis and discussion forums did not occur in some regions. Furthermore, some of these actions were taken as recently as 2021, a long time after the department committed to better coordination.
39. Recommendation. The Department of Health and Social Services and the health and social services authorities, in collaboration with Indigenous governments, communities, and service providers, should work to improve the coordination of addictions services across the territory by
- creating formalized referral processes to help connect clients to the required services
- evaluating the key positions that can facilitate referrals across services and where these should be located
The department’s and the health and social services authorities’ response. Agreed
See the List of Recommendations at the end of this report for detailed responses.
The department and the health authorities did not take sufficient action to ensure that addictions services were culturally safe
40. We found that the Department of Health and Social Services and the health and social services authorities did not take sufficient action to ensure that addictions services were culturally safe for Indigenous residents. Limited action was taken to remove barriers to cultural safetyDefinition 4. For example, we found that traditional Indigenous systems of experience and expertise were not recognized in hiring processes. We also found that policies were not reviewed to ensure that they supported a culturally safe system.
41. The analysis supporting this finding discusses the following topic:
42. This finding matters because Indigenous people in the Northwest Territories disproportionately face challenges with addictions. Increased cultural safety removes barriers to accessing services and helps to counter the effects of colonialism on the services that are available and on the way that they are delivered. This increases the likelihood that addictions services will meet the needs of Indigenous clients and help them achieve their recovery goals.
43. Indigenous people disproportionately experience negative health and social outcomes when compared to non‑Indigenous people in Canada. According to the Department of Health and Social Services’ 2017 and 2018 data, Indigenous residents are
- almost 6 times more likely than their non‑Indigenous peers to be hospitalized due to substance use
- about 3 times more likely to smoke
- about 1.5 times more likely to drink heavily
44. The Indigenous peoples of the Northwest Territories are not a single, homogenous group. They represent several different cultures, including (but not limited to) various Dene subgroups, Métis, and Inuvialuit. Part of the Government of the Northwest Territories’ commitments to provide health and social services includes working to ensure that all aspects of health and social services are culturally safe for everyone.
45. The 2016 document, Building a Culturally Respectful Health and Social Services System, included cultural safety best practices that the department had identified and commitments to how to improve the cultural safety of the health and social services system, including addictions services. These related to developing and reviewing policies, increasing workforce diversity, training staff, and incorporating traditional knowledge.
46. Our recommendation in this area of examination appears at paragraph 55.
Limited efforts to ensure cultural safety of addictions services
47. We found that the Department of Health and Social Services and the health authorities did not take sufficient action to ensure that addictions services were culturally safe for Indigenous residents.
48. We found that the human resources strategy for the health and social services system did not address how to increase the number of Indigenous employees in the system, a best practice that the department had identified in its commitment to cultural safety. Additionally, we found that neither the department nor the health authorities knew how many residents used the Government of the Northwest Territories’ programs targeted at encouraging local residents to seek employment in the system. This limited their ability to know whether they needed additional measures to facilitate increased Indigenous and local representation. At the time of our audit, the Northwest Territories Health and Social Services Authority was updating its 2015 human resources strategy.
49. We also found that neither the department nor the health authorities considered how to recognize traditional Indigenous systems of experience and expertise when hiring for positions in addictions services. Instead, they remained focused on the need for applicants to have formal post‑secondary education that results in Western-style qualifications. The focus on this type of education creates a barrier to employment for many Northwest Territories residents.
50. Related to this, we found that the department and the health authorities did not incorporate traditional Indigenous knowledge into measures to determine whether their services were helping clients achieve their desired outcomes (see paragraph 64). Some Indigenous organizations told us that they felt that department officials did not adequately understand Indigenous cultures and traditions.
51. We also found that the department did not try to measure the cultural safety of most addictions services until it launched the Addictions Recovery Survey in 2021, during our audit. Furthermore, we found that the department’s attempts to measure the cultural safety of the Community Counselling Program through client surveys were not effective because they did not collect information on the clients’ ethnicity. The results of surveys conducted in 2016 and 2018 indicated that more than 90% of respondents felt that their counsellor respected their culture, needs, preferences, or values. However, without information on clients’ ethnicity, the department did not know if this finding applied to Indigenous clients. At the time of our audit, the department was running another Community Counselling Program survey that asked clients to specify whether they were Indigenous, but it did not ask which Indigenous group clients were from.
52. We also found that the department did not review policies to ensure they reflected the cultural safety of addictions services, a commitment made in 2016. We noted that the new Community Counselling Program standards and operating procedures, approved in May 2021, provided direction to promote cultural safety. Other than this, the health authorities did not have policies on cultural safety, which would have reinforced its importance.
53. In 2019, the department released the Caring for Our People: Cultural Safety Action Plan, 2018–2020, which included a vision for the health and wellness of Indigenous people in the Northwest Territories and identified specific actions that would be taken in the health and social services system. The action plan stated that it was based on community collaboration. We found that the department’s own tracking of progress on this action plan indicated that the majority of actions were still in progress. While we recognize that improving cultural safety in the health and social services system is a significant undertaking that takes time, only a few of the action items identified in 2019 were indicated as completed by the department at the time of our audit.
54. However, we found that the department and 2 health authorities took some positive steps related to cultural safety:
- The department established the Indigenous Advisory Body to provide advice and guidance on the health and social services system.
- The department created the Community, Culture and Innovation Division within the department that would lead work on cultural safety. At the time of the audit, staffing of this division was still in progress.
- The department and 2 regions of the Northwest Territories Health and Social Services Authority provided some cultural safety training in addition to the mandatory cultural training that all Government of Northwest Territories employees must take.
- Since 2020, the Tłı̨chǫ Community Services Agency and 1 region of the Northwest Territories Health and Social Services Authority each created a position to support cultural safety of services in the communities they served. We were informed that as of July 2021, the Tłı̨chǫ Community Services Agency had not yet been successful in staffing its position.
55. Recommendation. The Department of Health and Social Services and the health and social services authorities, in collaboration with Indigenous communities and governments, should work to improve the cultural safety of addictions services. This should include
- reviewing their policies to identify any barriers to delivering culturally safe addictions services and working to remove these barriers
- developing and implementing a strategy to adapt its current hiring approach to formally recognize the value of Indigenous qualifications
The department’s and the health and social services authorities’ response. Agreed.
See the List of Recommendations at the end of this report for detailed responses.
Measuring outcomes for clients
The department and the health authorities did not know whether addictions services were effective
56. We found that the Department of Health and Social Services and the health and social services authorities did not know whether their addictions services were effective in helping residents achieve their desired outcomes. They did not sufficiently measure clients’ outcomes or use data to analyze trends.
57. The analysis supporting this finding discusses the following topic:
58. This finding matters because without measuring the performance of addictions services, the department and the health authorities cannot know whether the system helps clients achieve their goals or where to make changes to improve services for residents. Measuring performance would also help the department and the health authorities know if funds are being used in the most effective way. Thus, it is critical that the department and the health authorities collect and analyze relevant information to ensure that services are being delivered as required and that they measure and understand the results being achieved.
59. Our recommendations in this area of examination appear at paragraphs 66 and 67.
Client outcomes not measured
60. We found that neither the Department of Health and Social Services nor the health authorities collected or analyzed targeted data to expose trends about outcomes for clients, including those from diverse subpopulations. Instead, data collection and analysis were limited to periodic reviews of aggregated data. This was despite the fact that monitoring and evaluating outcomes had been identified as a priority area for action in the 2016 strategic framework for mental health and addictions.
61. We found that neither the department nor the health authorities analyzed Community Counselling Program data to identify clients’ outcomes. Program data was stored in paper-based client files and was never compiled in a disaggregated way to facilitate this type of analysis. Officials from the department and the Northwest Territories Health and Social Services Authority told us that they used aggregated Community Counselling Program data to identify trends and provide the rationale for new services. Beginning in the 2020–21 fiscal year, the Northwest Territories Health and Social Services Authority and the Hay River Health and Social Services Authority collaborated on a database that they could use to capture disaggregated client data. At the time of our audit, this database was in the pilot stage of implementation.
62. We found that the department did collect disaggregated data about clients who accessed facility-based addictions treatment, but it did not routinely analyze it. We analyzed this data and found trends that the department may want to explore to better understand the factors that can lead to improvements in service delivery and assessment. For example, the percentage of clients in facility-based addictions treatment from one Indigenous group was almost twice as high as its percentage of the general population. We also found that the department was aware of the number of individuals who did not finish treatment and, as part of its 2021 Addictions Recovery Survey, was trying to understand the reasons why. Targeted analysis of these trends might help to inform services.

Ensure healthy lives and promote well‑being for all at all ages
Source: United Nations
63. We also found that the department reported information related to 2 of the indicators for the United Nations’ Sustainable Development Goal 3: the harmful use of alcohol and the prevalence of tobacco use. According to the department’s 2019–20 annual report, results from Statistics Canada’s Canadian Community Health Survey indicated that in the 2017–18 fiscal year, the proportion of Northwest Territories residents who reported heavy drinking was 29% and the proportion who reported daily or occasional smoking was 35%. These results reinforce the importance of collecting and analyzing disaggregated data to understand how well addictions services are working and the changes that are required.
64. Additionally, we found that the department did not establish outcome indicators specific to most of its services. Before 2021, the department only measured outcomes for 2 of its services: the Community Counselling Program and an awareness campaign. For the counselling program, the department conducted a periodic survey of clients to determine their satisfaction on 2 measures: clients’ satisfaction with the overall changes in their lives since starting counselling and their satisfaction with changes to the original concern that brought them to counselling. In 2021, for the first time, the department also administered an addiction recovery experiences survey to clients who had accessed addictions services. It included a question on whether clients were satisfied with overall changes in their lives.
65. None of the health authorities measured outcomes for addictions services, except for the Hay River Health and Social Services Authority. It measured outcomes for 1 of its services in 2016.
66. Recommendation. The Department of Health and Social Services and the health and social services authorities should determine the disaggregated data required to understand whether addictions services are working, including for diverse subpopulations, collect and analyze the data to identify trends or anomalies, and use this information to adjust services as needed.
The department’s and the health and social services authorities’ response. Agreed.
See the List of Recommendations at the end of this report for detailed responses.
67. Recommendation. The Department of Health and Social Services and the health and social services authorities should collaborate with Indigenous governments and communities to establish desired short-, medium-, and long‑term outcomes for addictions services and indicators to measure them, including using Indigenous outcome measures. They should use these indicators to monitor the results related to addictions services and adjust those services as necessary.
The department’s and the health and social services authorities’ response. Agreed
See the List of Recommendations at the end of this report for detailed responses.
Conclusion
68. We concluded that despite commitments in the areas of equitable access, coordination of services, and cultural safety of services, the Department of Health and Social Services and the health and social services authorities did not do enough to provide addictions prevention and recovery services to meet the needs of Northwest Territories residents.
69. Neither the department nor the health authorities determined how they would provide equitable access to addictions services for residents. Thus, it was unclear whether the variability of addictions services over time and by location was part of the health and social services system’s design or due to deficiencies in the system. Furthermore, we found gaps in the coordination of services across providers 2 decades after the department committed to better coordinate the health and social services system to improve residents’ access to services.
70. The department and the health authorities also did not take sufficient action to ensure that addictions services for Indigenous residents were culturally safe or to know whether their addictions services were effective in helping residents achieve their desired outcomes.
About the Audit
This independent assurance report was prepared by the Office of the Auditor General of Canada on addictions prevention and recovery services in the Northwest Territories. Our responsibility was to provide objective information, advice, and assurance to assist the Northwest Territories Legislative Assembly in its scrutiny of the government’s management of resources and programs, and to conclude on whether the Department of Health and Social Services and the health and social services authorities complied in all significant respects with the applicable criteria.
All work in this audit was performed to a reasonable level of assurance in accordance with the Canadian Standard on Assurance Engagements (CSAE) 3001—Direct Engagements, set out by the Chartered Professional Accountants of Canada (CPA Canada) in the CPA Canada Handbook—Assurance.
The Office of the Auditor General of Canada applies the Canadian Standard on Quality Control 1 and, accordingly, maintains a comprehensive system of quality control, including documented policies and procedures regarding compliance with ethical requirements, professional standards, and applicable legal and regulatory requirements.
In conducting the audit work, we complied with the independence and other ethical requirements of the relevant rules of professional conduct applicable to the practice of public accounting in Canada, which are founded on fundamental principles of integrity, objectivity, professional competence and due care, confidentiality, and professional behaviour.
In accordance with our regular audit process, we obtained the following from entity management:
- confirmation of management’s responsibility for the subject under audit
- acknowledgement of the suitability of the criteria used in the audit
- confirmation that all known information that has been requested, or that could affect the findings or audit conclusion, has been provided
- confirmation that the audit report is factually accurate
Audit objective
The objective of this audit was to determine whether the Department of Health and Social Services and the health and social services authorities provided addictions prevention and recovery services to meet the needs of Northwest Territories residents.
Scope and approach
The audit included an examination of the department and the health authorities’ services to prevent and treat addictions, the coordination of those services, and how the services were monitored and measured.
The audit involved examining and analyzing key documents from the department and the health authorities. This included the files of 35 clients who attended a facility-based addictions treatment program at a facility in southern Canada between 2018 and 2021. These files were randomly sampled from the 3 health authorities. Our findings from the sample relate only to the files reviewed and are not meant to statistically represent the entire population of clients who attended facility-based addictions treatment. We also could not conclude on 3 of these files because of data integrity issues that we identified during the course of our work.
We interviewed officials in the department and in the 3 health authorities. We also had virtual interviews with several representatives from Indigenous governments and organizations to obtain their perspectives on the delivery of addictions services in the Northwest Territories.
The audit did not assess activities undertaken by other Government of Northwest Territories organizations, Indigenous governments, or other third parties that provide services. We also did not examine other areas of the health and social services system (for example, Child and Family Services).
We integrated questions about the United Nations’ Sustainable Development Goals into our audit approach. This reflects our commitment to do so in our Sustainable Development Strategy. We also looked at issues related to equity, diversity, and inclusiveness.
Criteria
We used the following criteria to determine whether the Department of Health and Social Services and the health and social services authorities provided addictions prevention and recovery services to meet the needs of Northwest Territories residents.
| Criteria | Sources |
|---|---|
|
The Department of Health and Social Services and the 3 health authorities provide equitable access to addictions services based on the needs of residents across the Northwest Territories in a culturally safe manner. |
|
|
The Department of Health and Social Services and the 3 health authorities integrate addictions services to ensure access and minimize gaps. |
|
|
The Department of Health and Social Services and the 3 health authorities monitor the delivery of addictions services, measure their performance and outcomes, and identify necessary adjustments. |
|
Period covered by the audit
The audit covered the period from 1 August 2016 to 31 July 2021. This is the period to which the audit conclusion applies. However, to gain a more complete understanding of the subject matter of the audit, we also examined certain matters that preceded the starting date of this period.
Date of the report
We obtained sufficient and appropriate audit evidence on which to base our conclusion on 1 March 2022, in Ottawa, Canada.
Audit team
This audit was completed by a multidisciplinary team from across the Office of the Auditor General of Canada, led by Jo Ann Schwartz, Principal. The Principal has overall responsibility for audit quality, including conducting the audit in accordance with professional standards, applicable legal and regulatory requirements, and the Office of the Auditor General of Canada’s policies and system of quality management.
List of Recommendations
The following table lists the recommendations and responses found in this report. The paragraph number preceding the recommendation indicates the location of the recommendation in the report.
| Recommendation | Response |
|---|---|
|
30. The Department of Health and Social Services and the health and social services authorities, in collaboration with Indigenous governments and communities, should determine how to achieve their commitment to providing equitable access to addictions services in the Northwest Territories, including related timelines, and take the required actions. This should include identifying where and how services should be made available to reduce barriers to access, given the operating environment and related challenges. |
Agreed. The Department of Health and Social Services and the health and social services authorities understand the importance of equitable access to addictions prevention and recovery services. In recent years, the department has invested heavily in reducing wait times and enhancing access to community-based addictions aftercare through the implementation of the Stepped Care 2.0 approach in the Community Counselling Program and the introduction of targeted community-based addictions recovery funding programs. In the 2022–23 fiscal year, the department will engage with Indigenous governments and communities on the topic of holistic mental wellness and addictions recovery supports to inform approaches to defining and achieving equitable access to addictions services. By the end of the 2023–24 fiscal year, and based on the results of the engagement work taking place in 2022–23, the Northwest Territories Health and Social Services Authority will work with the department and the health and social services authorities to develop a plan that outlines an approach to the locations of key addictions services and methods of delivery with a goal to reduce barriers where possible and within existing capabilities and system capacities. The health and social services authorities will then work to implement this plan. |
|
31. The Department of Health and Social Services, in collaboration with the health and social services authorities and relevant stakeholders, should identify the addictions prevention and recovery needs of diverse subpopulations. |
Agreed. The Department of Health and Social Services and the health and social services authorities recognize the importance of both the collection and thoughtful analysis of service user indicators to inform trends, profiles of individuals accessing services, and the needs and preferences associated with those distinct groups as it relates to addictions services. In the 2022–23 fiscal year, the department will determine an approach to the collection of service user experience and satisfaction data that includes additional demographic categories to capture the needs of diverse subpopulations, including refugee and non‑Indigenous racialized groups. In the 2023–24 fiscal year, the department will work with the health and social services authorities to combine the NWT Community Counselling Program Service User Satisfaction Questionnaire and the Addictions Recovery Experiences Survey (both most recently conducted in 2021–22) into one overarching Mental Wellness and Addictions Recovery Experiences Questionnaire. Included in this questionnaire will be the additional demographic categories identified in 2022–23, as described above. The results of the questionnaire will be used to inform departmental understanding of the addictions prevention and recovery needs of all Northwest Territories residents, including diverse subpopulations. This questionnaire will form an ongoing approach to data collection that will be administered every 2 to 3 years. |
|
35. The Department of Health and Social Services and the health and social services authorities should
|
Agreed. The Department of Health and Social Services and the health and social services authorities recognize the importance of aftercare plans that identify the individualized supports and resources necessary to celebrate successes, encourage healthy habits, cope with triggers, and work toward personal recovery goals. Aftercare planning is an important part of the work that health and social services professionals do with individuals seeking facility-based treatment, and it is recognized that there is a need to improve consistent documentation of this work in line with best practice. By the end of the 2022–23 fiscal year, working with the department and the health and social services authorities, the Northwest Territories Health and Social Services Authority will lead a review of current practices in aftercare planning and create a revised, standardized approach to aftercare planning that is reflective of established standards and best practice. This work will include the development of standardized tools and processes that will ensure a documented aftercare plan is clearly identified on the service user’s file prior to leaving for treatment. The approach will also ensure regular updates during treatment, proactive connection upon completion of treatment, and active outreach to ensure that residents accessing addictions treatment are connected to resources and set up for success upon returning to the Northwest Territories. |
|
39. The Department of Health and Social Services and the health and social services authorities, in collaboration with Indigenous governments, communities, and service providers, should work to improve the coordination of addictions services across the territory by
|
Agreed. The Department of Health and Social Services and the health and social services authorities recognize the importance of ensuring that every door is the right door when it comes to accessing addictions recovery services. Key to the successful implementation of this approach is integration of services and clear communication of the available resources and how to access them. Many addictions recovery services available to residents of the Northwest Territories are accessible through self‑referral, and it is recognized that residents require more clear communication of available services and how to access those services. By the end of the 2022–23 fiscal year, the Northwest Territories Health and Social Services Authority, in partnership with key stakeholders and with the support of Indigenous governments, the Leadership Council, and Regional Wellness Councils, will work with the department and the health and social services authorities to complete a gap analysis to identify areas requiring targeted quality improvement. This analysis will inform the development of standardized processes for both provider and self‑referrals that include key referral points and pathways to accessing addictions services. The health and social services authorities will then implement these referral processes. |
|
55. The Department of Health and Social Services and the health and social services authorities, in collaboration with Indigenous communities and governments, should work to improve the cultural safety of addictions services. This should include
|
Agreed. The Department of Health and Social Services and the health and social services authorities understand the importance of providing addictions prevention and recovery services that are culturally safe and free from racism. By the end of the 2023–24 fiscal year, the department and the health and social services authorities, with the support of established health and social service system advisory bodies, will conduct a review of standards and policies associated with key addictions services including the Community Counselling Program and the Facility Based Addictions Treatment Program to identify barriers to cultural safety. The results will be used to inform efforts to remove or reduce identified barriers. By the end of the 2023–24 fiscal year, the Northwest Territories Health and Social Services Authority will work with the department and the health and social services authorities, and with the support of established advisory bodies, to review and adjust screening processes, core competencies, and equivalencies for key addictions services positions to ensure the inclusion and application of Indigenous qualifications. |
|
66. The Department of Health and Social Services and the health and social services authorities should determine the disaggregated data required to understand whether addictions services are working, including for diverse subpopulations, collect and analyze the data to identify trends or anomalies, and use this information to adjust services as needed. |
Agreed. The Department of Health and Social Services and the health and social services authorities agree that there is room to conduct more thorough and targeted data analysis as it relates to the use of addictions prevention and recovery services by diverse subpopulations in the territory. By the end of the 2023–24 fiscal year, the department will work with the health and social services authorities to complete an examination of the ability to disaggregate program data based on current data collection approaches and the appropriateness of collecting data on additional demographic groups, including the lesbian, gay, bisexual, transgender, queerLGBTQ+ community, refugees, and non‑Indigenous racialized groups. This work will include a review of best practices, a feasibility assessment, and the compilation of an inventory outlining existing data collection across key addiction service areas. Following this, the department will determine an analytic approach for any additional categories that will be collected as part of ongoing program monitoring data for the Community Counselling Program and facility-based addictions treatment. The results of the analytic approach will be used to inform adjustments to services as necessary. |
|
67. The Department of Health and Social Services and the health and social services authorities should collaborate with Indigenous governments and communities to establish desired short-, medium-, and long‑term outcomes for addictions services and indicators to measure them, including using Indigenous outcome measures. They should use these indicators to monitor the results related to addictions services and adjust those services as necessary. |
Agreed. The Department of Health and Social Services and the health and social services authorities understand the importance of establishing indicators to track progress and outcomes over time. As the focus of service delivery shifts towards integration with community and Indigenous groups, the approach to the establishment of indicators and outcome measures must also shift. In the 2022–23 fiscal year, the department will work with the health and social services authorities and Indigenous governments and communities to inform the development of logic models and monitoring frameworks for the Community Counselling Program and other key addictions services, including community designed and delivered services. This work will identify short-, medium- and long‑term outcomes as well as key indicators and will embed applicable community-determined outcomes into the overall monitoring approach. The monitoring approach will be implemented in the 2023–24 fiscal year, and results will inform shifts in service delivery, as necessary and feasible. |